Here are the common misconceptions, the truth and the lies.
In the vast majority of cases in our team, we use hip prostheses combining an impacted (cementless) cup and an impacted (cementless) stem.
As soon as the femoral bone shows signs of fragility (osteoporosis), we prefer to use a cemented stem for greater safety (less risk of fracture or secondary sinking).
As far as the friction torque is concerned, in the majority of cases we use a ceramic-ceramic torque, but also a ceramic-Highly Crosslinked Polyethylene (XLPE) torque, or a dual mobility acetabular cup (particularly if we feel there is a higher risk of dislocation).
It should be noted that today's literature shows identical survival times (wear rates) between ceramic and highly cross-linked polyethylene.
In certain special cases, we may have to choose a made-to-measure hip prosthesis. This is particularly the case for patients with a constitutional bone disease (congenital disease) such as polyepiphyseal dysplasia, spondyloepiphyseal dysplasia, pseudoachondroplasia, certain forms of multiple exostoses, etc....
We may also have to choose a custom-made prosthesis for certain sequelae of childhood pathologies such as epiphysiolysis or primary osteochondritis of the hip.
Thus, the indications that seem to us to justify the use of a custom-made prosthesis are relatively limited.
Here are a few questions and answers (taken from questions asked by our patients) to clarify what is true and what is not, and to dispel preconceived ideas about "made-to-measure" hip replacements:
Question 1: "A made-to-measure hip prosthesis is entirely made to measure identical to my hip?" FALSE.
A hip prosthesis consists of two parts:
- 1° the prosthetic "cup" or "acetabulum" which is cemented or impacted (without cement) into the pelvic bone and
- 2° the femoral stem which is cemented or impacted (without cement) into the femoral bone and on which a ball is positioned which articulates with the cup.
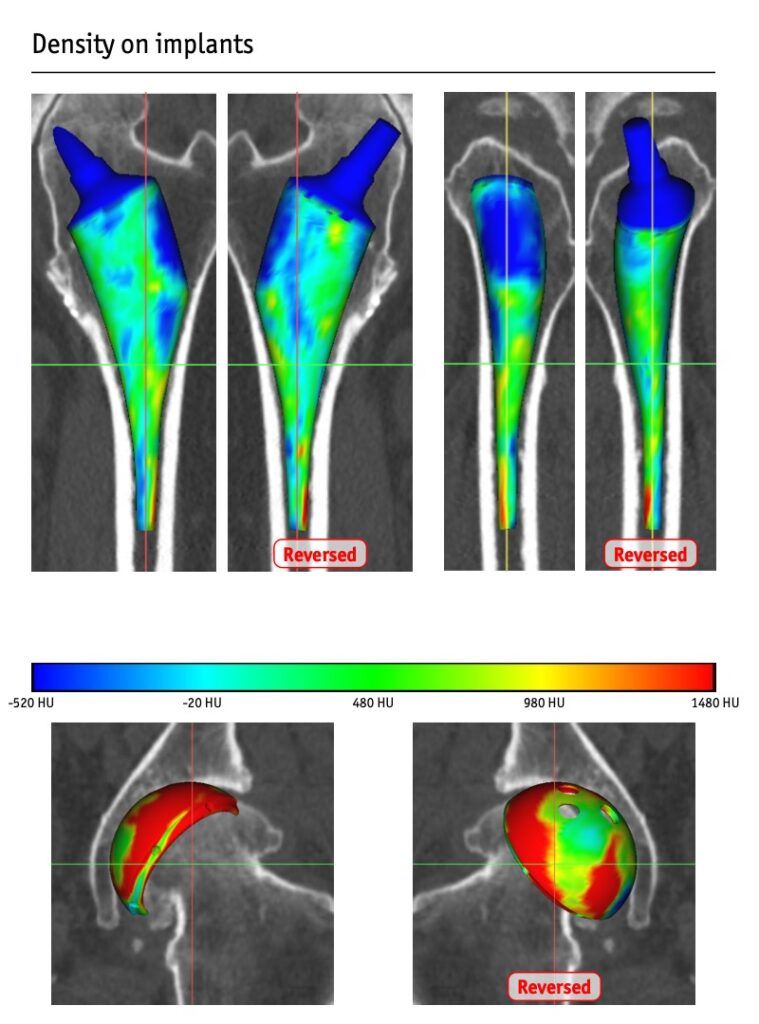
In a custom-made hip prosthesis, only the femoral stem is custom-made. It is designed using software based on a 3D scanner reconstruction. The stem manufactured in this way will take the shape of the inside of the femur bone to adapt as closely as possible to this bone, as shown in the figure below.
This implant can therefore be useful to the surgeon for positioning the stem in a very abnormal femur that has undergone a great deal of alteration. In the case of a congenital disease, for example, as mentioned above, or for extreme sizes. But this does not improve the performance of the patient's hip.
The neck of the made-to-measure stem theoretically restores the length and offset (lateralization) of the patient's hip joint.
But all these calculations can be modified and rendered inoperative during the operation by the positioning of the acetabulum. For one thing, the acetabulum is not made to measure, and it is not necessarily positioned exactly by the surgeon as expected by the CT planning.
Unfortunately, it is quite possible to make a length error with a made-to-measure hip prosthesis, or a lateralization error.
Question 2: "A custom-made hip prosthesis gives better results than conventional prostheses". FALSE
Based on our long experience of hip surgery and that of the colleagues we work with on a daily basis, we can say that there is no improvement in the results obtained with a made-to-measure hip prosthesis compared with a conventional hip prosthesis.
The same applies to the results reported in the international literature.
The post-operative course is the same, with the same instructions.
The types of sports and physical activity permitted are also the same. They depend essentially on the intrinsic capacities of our patients and the preservation of muscles and tendons during the operation.
Question3: "There is no dislocation with a made-to-measure hip prosthesis!" FALSE.
There is a risk of dislocation with a custom-made hip prosthesis, as with a conventional prosthesis. These risks are low, particularly if the operation has been carried out with care to preserve the muscles and tendons.
We believe that the anterior approach helps to reduce the risk of dislocation.
Good preoperative planning (using dedicated software) and compliance with this planning will ensure that the hip is stable and that the architecture of the hip is restored.
Qurestion 4: "You need a made-to-measure hip prosthesis if you want to take part in sporting activities, if you're an athlete...". FALSE
A made-to-measure hip prosthesis does not increase sporting performance. As with the risk of dislocation, the key to recovering from sporting activities is to preserve the muscles and tendons during the operation and fit a stable implant.
Question 5: "Can a made-to-measure hip prosthesis be useful? TRUE.
A made-to-measure hip prosthesis can help the surgeon and make his work easier in some of the situations I have already mentioned: a very abnormal femur, a femur that has been heavily reshaped, a very small or very large femur (in the extreme sizes) that exceeds the usual limits...
It's an interesting tool that needs to be used in the right way.
However, custom-made hip replacements should not be presented as the solution to all problems or as a way of avoiding all complications.


